Confronting COVID-19 Vaccine Inequity
Researchers at the Duke Global Health Institute are measuring global inequities in vaccine distribution -- and they have solutions

Ending the COVID-19 pandemic means vaccinating the whole world, and manufacturing billions of doses is just the start.
“An outbreak anywhere,” said Gavin Yamey, “can become an outbreak everywhere.”
Yamey is on one of several teams at DGHI, the Duke Global Health Institute, addressing the obstacles to equitable vaccine distribution around the world. The teams are creating tools to provide comprehensive information on vaccine supply, as well as the means to distribute that supply equitably around the world.
One barrier to equitable vaccine distribution is wealthy countries snapping up available supplies. That’s what happened in the H1N1 outbreak in 2009, when bigger countries made direct deals with vaccine manufacturers.
“I'm very sad to say that behavior has repeated itself,” Yamey said. “Rich nations are hoarding the vaccine.”
Yamey directs the Center for Policy Impact at DGHI. He and others including David McAdams, a professor at Duke’s Fuqua School of Business, have proposed a mechanism to reverse that trend.
“This race to develop vaccines around the world has the potential to become a zero-sum game, where something we do to benefit ourselves here in the United States might harm others by delaying their access to the vaccine,” McAdams said. “But it doesn't have to be that way.”
McAdams and Yamey propose incentives for wealthy nations to participate in COVAX, a new COVID-19 Vaccine Global Access Facility backed by the World Health Organization and others. COVAX plans to vaccinate a billion people by the end of 2021, basing vaccine distributions to participating countries on population.
The Duke professors found wealthier nations could make vaccine deals that help other countries without short-changing their own populations.
“There's several ways that can happen,” McAdams said. “But the most important is through transferring know-how and capabilities.”
McAdams and Yamey propose that purchase deals between wealthier countries and vaccine manufacturers require the vaccine makers to share the knowledge and technologies with other manufacturers with available capacity so they can produce the vaccine for less wealthy countries.
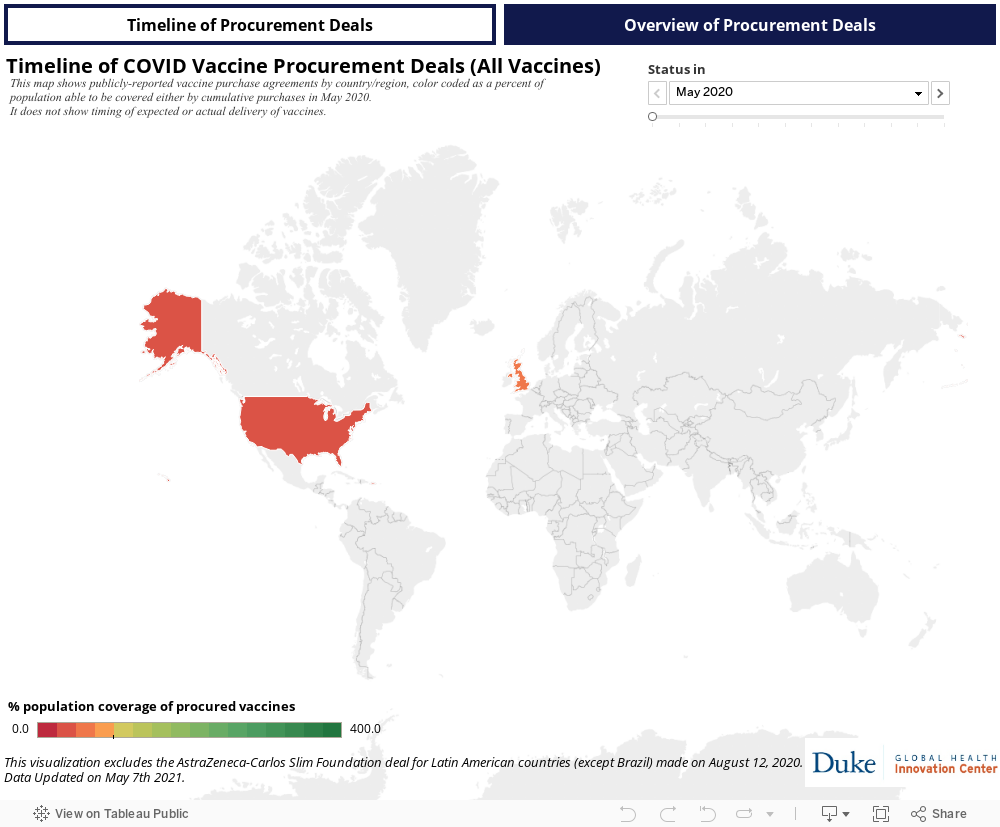
In past pandemics, it wasn’t clear exactly how many vaccine doses were ending up in which countries. But the Duke Global Innovation Center, part of DGHI, has helped clarify that picture. The Center compiles and analyzes publicly available data on COVID-19 vaccine manufacture and procurement as part of its Launch and Scale Speedometer project.
The indicator was created in 2019 to track scaling up of health care innovations in low-to-middle income countries. When COVID hit, the creators switched to monitoring nations’ vaccine purchases.
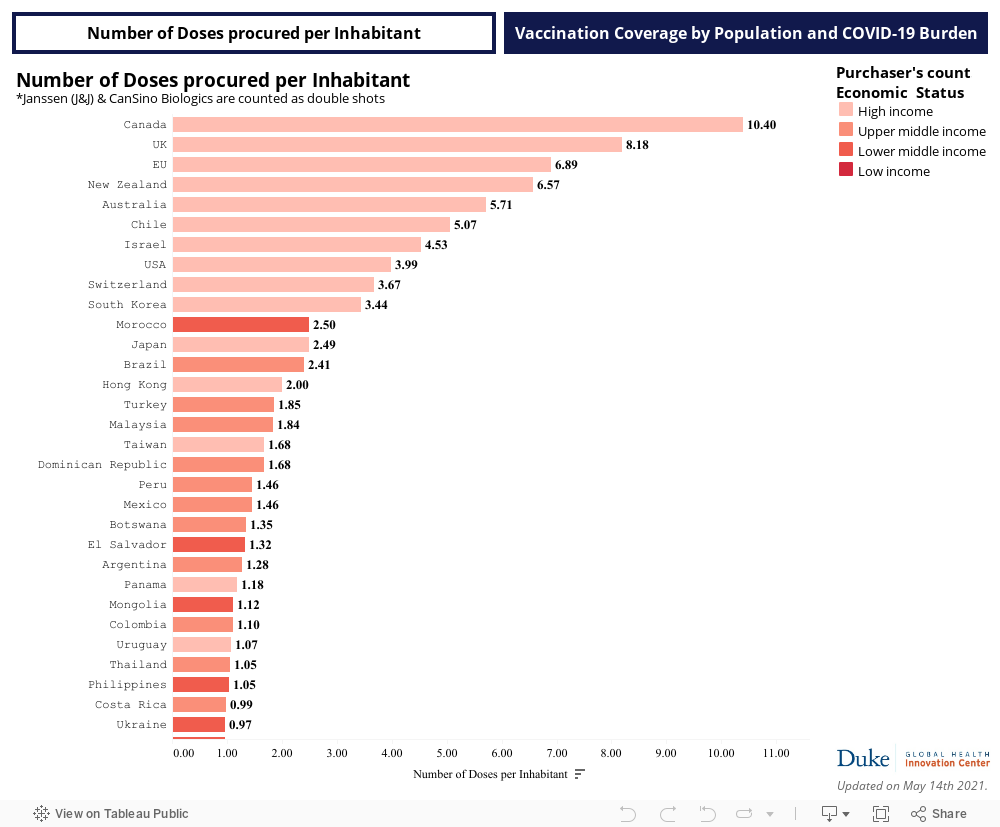
“Before vaccines were even on the market, we saw an unprecedented number of advance purchases,” said Andrea Taylor, who leads the COVID-19 aspect of the speedometer project.
“We can see there is a very large gap that is developing,” Taylor said. “We’re particularly concerned about the countries facing high COVID burdens that aren’t anywhere near 100 percent population coverage with their vaccine orders.”
The Speedometer started small, but quickly drew strong interest from governments and others.
“The purpose we're serving is not just a tracking tool, but also to make sure that we're sharing the lessons learned around the challenges to equitable distribution and helping to guide decision-making by global health bodies, countries and manufacturers,” said Krishna Udayakumar, founding director of DGHI’s Innovation Center.
That’s already starting to happen in Canada, which the Speedometer showed had purchased the most vaccine doses per capita. The Canadian government has since indicated it will work with COVAX to ensure any surplus doses are used equitably.
“Those are some of the conversations we’re helping to influence,” Udayakumar said.
Beyond ensuring supply is shared, countries each face logistical challenges to getting their populations vaccinated.
Osondu Ogbuoji – an assistant research professor at DGHI who is also involved in the equitable distribution work – is leading a team identifying vaccine distribution bottlenecks. The goal is to craft concrete steps health systems can take to build the capacity they need.
“Little is being done to address country-level capacity to cope with the financing and logistic challenges needed to deliver on this unprecedented effort,” Ogbuoji said.
Meanwhile, João Ricardo Vissoci, an assistant professor of surgery, leads a team developing an open-source platform that uses artificial intelligence to estimate target populations for vaccination campaigns. And Professor Shenglan Tang, a professor of population health science at Duke and deputy director of DGHI, is part of a team supported by the Gates Foundation that is compiling field data to fuel policy recommendations for the Chinese government’s vaccine distribution plans.
Governments leaders have a natural tendency to want to protect their own people first. Yet it’s in every government’s interest to make sure other countries get a fair share, Udayakumar said.
“The humanitarian and ethical argument for equity is strong on its own, but models also show clearly that the number of deaths that can be prevented are much higher with equitable distribution,” he said.
“There are also models that show economic growth in high-income countries will be higher in the coming years if we take the more equitable approach to vaccine distribution.” Udayakumar said. “So I think there are some positives to take away, but clear warning signs about the path forward.”