
Jeffrey Lawson, MD, PhD, holds out one hand, palm flat and fingers pointed straight up, and slowly raises it straight toward the ceiling. "It was like watching a rocket take off," he says. "You stand there watching it go up, and then ..." His hand reaches eye level, and then slows, traces an arc, and plummets back toward the floor. "Boom."
Lawson looks up and smiles. "Back to the drawing board," he says.
The remarkable journey of discovery taken by Lawson, a vascular surgeon and biologist, and his former Duke colleague Laura Niklason, MD, PhD, to successfully create and implant a bioengineered blood vessel included more such back-to-the-drawing-board moments than the researchers can count.
But each one of those hurdles -- each chemical formulation that lacked sufficient cohesion, each attempt that failed to grow the requisite cell layers, each animal prototype that ruptured under stress -- taught them something.
And each of those lessons was a stepping stone that ultimately led to the first successful implantation of a bioengineered blood vessel in a human being by a Lawson-trained surgical team in Poland in late 2012, and the day in June 2013 when Lawson stitched a bioengineered blood vessel onto the artery of a Virginia hemodialysis patient named Lawrence Breakley in a Duke University Hospital operating room, the first such procedure in the United States.
The accomplishment shows every sign of being one of those rare breakthroughs that represents a truly new horizon in medicine. Building on the work Lawson and Niklason have done, it's hard not to envision a future when not only blood vessels but all sorts of replacement tissues and organs may be grown from human cells in the lab, stored indefinitely on the shelf, and then transplanted into patients when needed.
"This is a paradigm shift," says Niklason, who was on the faculty at Duke until 2006 and is now a professor of anesthesiology and biomedical engineering at Yale. "To the best of my knowledge nobody else in the world has done this, and certainly nobody has taken it into the clinic. This opens a lot of doors."
The world at large recognized that immediately. Breakley's surgery made headlines throughout the country and across the globe, and in the weeks and months afterward Lawson and Niklason found themselves giving interviews to journalists from places as diverse as Iran, Greece, and Brazil.
"I expected some attention, but honestly, probably not quite as much as we've gotten," says Lawson. "But it is an intriguing story for a lot of reasons, from human interest to medical technology, to a good message about advances in biomedical research. People are fascinated by the fact that we're making human tissues."
Even after all these years of working on the project, Lawson and Niklason are among those people.
"Sometimes I pinch myself and think, 'Wow, I get to be a part of all of this,'" Lawson says.
For her part, Niklason says, "It's been 18 years of hard work, but it still seems sort of amazing that it works."
AN IMMENSE CLINICAL NEED
The surgery to implant the new blood vessel in Breakley's arm took just two hours, but it represented the culmination of almost two decades' worth of work and research. Lawson and Niklason teamed up in the late 1990s when they discovered grafting blood vessels.
The need was, and is, immense; every year many hundreds of thousands of patients in the U.S. require replacement of blood vessels for heart bypass, hemodialysis, peripheral artery disease, and other conditions.
The standard process is to graft either veins taken from elsewhere in the patient's own body or synthetic blood vessels onto the affected artery.
Both procedures are fraught with problems. Many patients don't have sufficiently robust or healthy veins to harvest. Veins and arteries are structurally different organs, and using veins to do the job of arteries seldom works very well. And, even in the best cases, harvesting a patient's own veins requires an additional surgical procedure, with another incision site, and increased operative time, cost, recovery period, and potential for complications.
Synthetic blood vessels are prone to clotting, rejection, and other complications.
"Natural blood vessels work in a way that is very different from a plastic tube, and an artery is very different from a vein," says Lawson. "Laura and I, from different perspectives -- me from the surgical perspective and she from her experience as an anesthesiologist watching surgeons struggle to harvest veins -- both came to the conclusion that there has to be a better way."
Niklason began working on that problem as a post-doc at the Massachusetts Institute of Technology.
"I remember watching surgeons dig around in the legs or abdomens of patients trying to get veins for bypass," she said. "I thought, 'This is sort of a barbaric process. Do we not know enough about blood vessels to grow our own in the lab?'"
TRIAL AND ERROR
Shortly after Niklason arrived at Duke in 1998, she and Lawson met over an operating table and soon discovered their shared interest in improving vascular grafts. They joined forces to build on the work she had begun. Although some bioengineered tissues had been developed at the time, the idea of growing blood vessels from human cells was still "a little bit out there on the lunatic fringe," Niklason says.
In Lawson, she found the perfect collaborator, and at Duke, the perfect institution.
"Her background is in bioengineering, mine is in vascular biology, so we had different but complementary skill sets," Lawson says "And at Duke we were in an environment that allowed us to collaborate, and we had supportive departments that allowed our collaboration to flourish. For a project this complex, you require that interdisciplinary, multi-faceted approach. We've probably had 20 or 30 grad students, medical students, and post-docs working with us along the way."
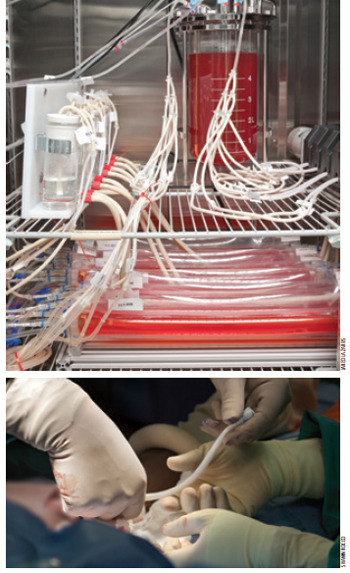
By the time she got to Duke, Niklason had developed a workable version of the first essential component: a biodegradable "scaffolding," a tube-shaped mesh structure that could be made in various lengths and widths. The idea was to "seed" smooth muscle cells onto the scaffolding and immerse it in a stew of amino acids and other nutrients within a "bioreactor," a container that would mimic the temperature and environment inside the human body where cells naturally grow.
The cells would grow and adhere together -- "It's basically like growing grass seed," says Lawson -- and the scaffolding would dissolve, ultimately leaving behind a solid, flexible tube made of muscle tissue.
It's easy to visualize, but it was very difficult to do. Every step -- creating a scaffolding that would support the structure but dissolve at the right rate, developing the bioreactor, finding the right combination of nutrients to grow the cells -- required a laborious process of trial and error.
"There was a lot of tinkering, a lot of prototyping," says Lawson. "It was, 'Let's add more Vitamin C, let's try this or that.' Each one was like, 'Put a little more salt in the sauce.'"
They experienced, Niklason says, "a very large number of failures. But bit by bit we solved the problems."
A COUNTERINTUITIVE BREAKTHROUGH
After many attempts and adjustments they came up with a process that consistently produced arteries strong and stable enough to function properly when implanted in pigs. Once they had solved that challenge, though, the researchers found themselves facing another. They had proven that they could grow a new blood vessel from an animal's cells and successfully implant it into the same animal. But from a practical standpoint, doing the same thing in humans posed a big problem.
"We could make your own blood vessel for you, but we needed a three to four month lead time -- and if you need a heart bypass or a bypass around a circulation blockage in your leg, you usually don't have four months to wait around for it," Lawson says. "We needed to be able to grow them in batches and have them available. Growing them from the host one at a time isn't going to work. But at the same time, if we make the structure from your cells and put it in me, my body would identify it as foreign. How do we make it universally transplantable? OK, back to the drawing board."
The answer was deceptively simple, if somewhat counter-intuitive.
They devised a process by which, after growing a vessel from a donor's healthy cells, they "decellularize" it, washing it in a solution that rinses away the living cells. What is left is a flexible tube of collagen that is immunologically neutral.
"It's still a tissue, but it's non-living, so it doesn't trigger an immune response," Niklason said. "That means we can store it for months, and if somebody needs an artery we can take it off the shelf and put it in the same day."
What they found next, when they implanted the new blood vessels in baboons, was in some ways the most remarkable aspect of the whole project. Not only does the host's body not reject the new blood vessel as foreign -- the body's own cells quickly start to populate the new vessel, like new people moving into an empty building.
"To me, that's the most exciting, fascinating, science fiction-y part of this whole thing," says Lawson. "Within a few weeks, it's no longer our structure at all. It's your blood vessel, made up of your tissue. It becomes a part of you."
INTO THE OPERATING ROOM
By 2012, after a series of successful trials in baboons, the researchers were confident they had developed a technology that would work and would prove superior to the existing methods of vascular grafts. They applied for regulatory approval to begin human trials in both the U.S. and in Poland, and Niklason founded a spinoff biotechnology company called Humacyte to manufacture the blood vessels in quantity in 2005.

The Polish regulatory mechanism moved more swiftly than the one in the U.S. Teams of Polish surgeons came to Duke to operate with Lawson, and he went there to oversee the procedures, and in December 2012, a team of surgeons from Poland implanted a bioengineered blood vessel in the first human patient. Since then, 20 other implants have been done at three sites in Poland.
"I remember saying at the time that this represents 15 years of Duke-supported research from multiple departments and multiple investigators," says Lawson.
Several months later the FDA signed off on U.S. trials, and Duke gave its go-ahead. Lawson selected Lawrence Breakley, a 62-year old man from Danville, Va., with end-stage renal disease, for the first U.S. procedure. He is one of the 350,000 people in the nation who needs hemodialysis, a thrice-weekly procedure that draws blood, filters toxins out of it, and then returns the cleansed blood to the system. Prior to the bioengineered vessel graft, Breakley was out of options: both natural and synthetic grafts in him had failed.
"Dialysis is the safest place to test emerging vascular technologies, because it meets the fundamental requirements for what you need a blood vessel to do, but if it fails you don't lose your leg or have a stroke or a heart attack," says Lawson. "If it fails or shows any sign of weakness or rejection, we'll be able to see that and deal with it, because it's right under the skin, not deep in your leg or in your chest cavity."
On June 5, 2013 -- in Operating Room (OR) 17 at Duke University Hospital, the same OR where Lawson and Niklason first met 15 years earlier -- Lawson grafted a length of bioengineered blood vessel onto an artery in Breakley's arm. By all indications, it was a complete success.
"It's amazing, you know, the things they can do," Breakley told a local newspaper after the operation. "At the rate they're going, eventually there won't be any part of the body they won't be able to give (patients)."
THE RIGHT TREE
Lawson followed the initial operation up with several more in the following weeks, with still more on the way.
Thus far, all indications are that the grafts done both in Poland and in the U.S. are working just as the researchers projected they would. Assuming the grafts in dialysis patients' arms continue to function without complications, the plan is to begin using the new blood vessels to treat peripheral artery disease (PAD) and then, at some point in the future, for coronary bypasses.
And ultimately, Niklason says, the potential exists to use the same technology to grow many other sorts of tissues -- for respiratory, gastrointestinal, and urinary tracts, for example.
But one step at a time, she cautioned. What the researchers have already accomplished is breathtaking.
"It's gratifying and exciting and scary all at the same time," says Niklason. "If you work on something your whole adult life and now it's being tested, you hold your breath a little bit. It has huge implications for the patients, obviously, because we want them to do well. But it's also the moment when you find out whether you've been barking up the right tree this whole time. And so far, it looks like we have."
NEXT STEPS
That doesn't mean the hurdles are over. Probably the biggest immediate challenge is economic: Can bioengineered blood vessels be manufactured and implanted at a cost that will make them widely available in the health care marketplace? That is a tremendously complicated equation, involving production scale, up-front costs versus long-term savings, competition from synthetic vessel manufacturers, and many other factors.
"You can make the coolest, fanciest thing, but if it's unobtainable with the health care dollars we have, it will die an economic death," Lawson says. "I wouldn't be talking to you if I didn't think it was going to work, but the biggest challenge in the next two to five years will be the business model viability."
As Lawson describes the long journey and the many hurdles the researchers had to overcome, he shakes his head in wonder at how many times an idea that seemed a little off the wall at the time turned out to the be the solution.
"So many of these breakthroughs were dumb-luck things," Lawson says with a smile.
"Somebody says, 'Hey, how about we try it this way?' 'OK, give it a shot!' That's the nature of research. I love that quote from Albert Einstein: 'If we knew what we were doing, it wouldn't be research.'"
And they aren't done yet. In some ways, with the trials under way, the next series of procedures on the horizon, and Humacyte working on the manufacturing and business end, they're just setting out.
"Laura and I sometimes tease other," says Lawson. "We tell each other, 'Fifteen years down the road, we're at the end of the beginning.'"